Madeeha Laghari,
Yusrida Darwis ![]() ,
Abdul Hakeem Memon,
Arshad Ali Khan,
Ibrahim Mohammed Tayeb Abdulbaqi,
Reem Abou Assi
,
Abdul Hakeem Memon,
Arshad Ali Khan,
Ibrahim Mohammed Tayeb Abdulbaqi,
Reem Abou Assi
For correspondence:- Yusrida Darwis Email: yusrida@usm.my Tel:+6046532211
Received: 23 June 2015 Accepted: 30 November 2015 Published: 29 January 2016
Citation: Laghari M, Darwis Y, Memon AH, Khan AA, Abdulbaqi IM, Assi RA. Nanoformulations and clinical trial candidates as probably effective and safe therapy for tuberculosis. Trop J Pharm Res 2016; 15(1):201-211 doi: 10.4314/tjpr.v15i1.28
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Tuberculosis (TB) is the main infectious disease causing 1.8 million deaths worldwide every year and represents a principal cause of mortality resulting from a bacterial infection. The emergence of multidrug-resistant strains and lack of effective anti-TB drugs are threatening the future control of TB. The present multidrug regimen against TB needs daily administration for at least 6 months, and patients often fail to follow this complex regimen for such a long interval, thus leading to patient non-compliance and treatment related side effects. To avoid daily dosing, application of nanotechnology is a promising solution by virtue of sustained drug release. Nanotechnology-based rational targeting may improve therapeutic success by limiting adverse drug effects and requiring less frequent administration regimens, ultimately resulting in higher patient compliance, and thus attain higher adherence levels. Today, the pipeline of potential new treatments consists of several compounds in clinical trials or preclinical development with promising activities against sensitive and resistant Mycobacterium tuberculosis strains. Encapsulation of existing anti-TB drugs into nano-delivery systems and introduction of new drugs in combination treatment for all forms of tuberculosis have resulted in novel treatments with more effectiveness and reduced side effects.
Introduction
Tuberculosis (TB) is one of the significant contagious diseases worldwide and its frequency is increasing principally in association with AIDS pandemic. TB is not an addition in the recently discovered array of diseases but an ancient human disease that dates back to decades, however still it can be enumerated as one of the most prevalent and life threatening disease [1]. Despite the accessibility to cost saving and effective medication, TB is still held responsible for countless cases of active diseases and innocent avoidable deaths worldwide [2].
Unfortunately, the heartbreaking failure is the inability to cope up with the prevailing drug resistant strains of TB, examples of which are multi drug resistant (MDR) TB and extensively drug resistant (XDR) TB which are acutely adverse and life threatening [3]. Due to wide spread MDR-TB strains, world has encountered painful failure in wiping away this disease completely. It has been generally determined that patients without a fragment of hope and totally down-hearted may not continue the therapy because of side effects, prolong treatment, or relief of the symptoms.
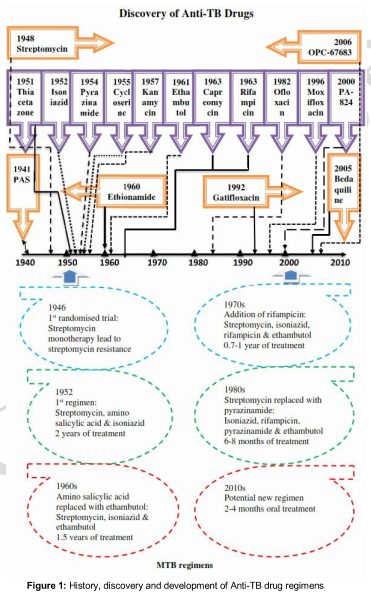
Strictly speaking, TB is one of such unfortunate diseases for which very limited antibiotics are discovered and very few are in pipeline. shows some of the major milestones in the discovery and development of drugs and regimens for TB. Rifampicin (RIF), isoniazid (INH), pyrazinamide (PYZ), and ethambutol (EMB) are the primary most choices for the clinical disease management. Internationally acknowledged 90 % efficient, authentic treatment of active tuberculosis with HIV dormant consists of 6 months chemotherapy regimen using a combination of 4 drugs (RIF, INH, EMB, PYZ) daily for two months followed by RIF and INH for 4 months either daily or three times per week [4].
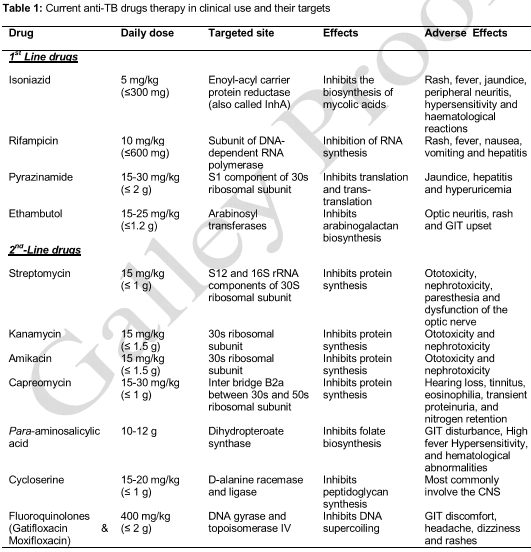
First line therapy is a refined combination of these 4 drugs with addition of streptomycin (STR). For more advanced complex drug resistant strains MDR-TB and XDR-TB, suggested treatment includes the recommendation of any fluoroquinolone, together with at least one of three second-line injectable anti-TB drugs i.e. amikacin and capreomycin [5]. Targeted sites, doses, pharmacological and adverse effects of anti-TB drugs are summarized in .
Treatment of TB is composite and is becoming more and more composite with the emergence of MDR and HIV infection. Daily administration of combined antibiotic therapy of TB for at least six months may cause the early ending of treatment due to side effects or alleviation of primary symptoms which may lead to MDR-TB and XDR-TB. Drug delivery systems using encapsulation technology is likely to perform its role by formulating anti-TB drugs into sustained release systems. Hence, encapsulation of current anti-TB drugs into nano delivery systems should be viewed to increase drug concentration at infected sites, improve their therapeutic index, reducing toxic effects and extent of treatment [6].
The aim of the present review is to highlight the potential advantages of these nanoparticles significant to the treatment of TB. Moreover, the safety and efficacy of new drugs in addition to an optimized standard therapy for the treatment of multidrug-resistant TB, also discussed.
NANO CARRIER SYSTEMS
Nanotechnology and nano science studies are a warm-heartedly welcomed revolution in a modern era of advancement. These studies have dramatically emerged during the last few decades in a vast field of product domains and have captured enormously generous attention due to their compact size properties [7].
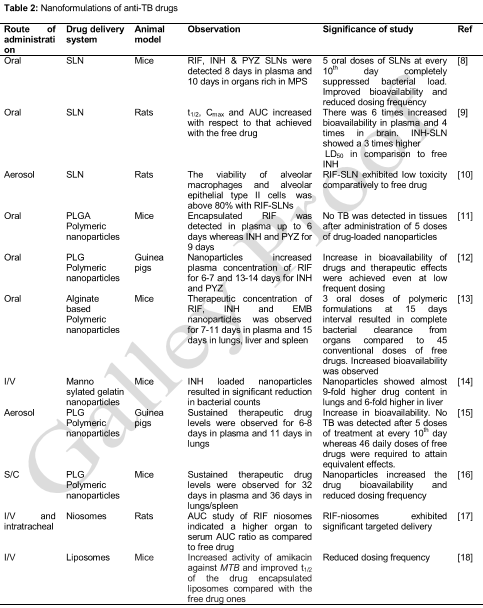
Nanoparticle-based delivery systems propose a number of advantages and give way to a bright possibility of introducing different routes of drug administration for better management of the disease. Numerous attempts have been made by scientists to encapsulate anti-TB drugs into different types of nanoparticles. These formulations have shown better results in terms of bioavailability, dosing frequency, safety and duration of treatment when compared with standard therapy .
Types of nanoparticles
(i) Liposomes
Liposomes are accurately best defined as tiny spherical lipid globules with a bi-layered membrane structure consisting of natural or synthetic amphiphilic lipid molecules with an aqueous interior [19]. Liposomes are taken up by macrophages, release their contents intracellularly, and are effective against intracellular pathogens, e.g., M. tuberculosis. Deol et al developed liposomes (Stealth®) which were more effective than free drugs for targeted delivery to the lungs. The free INH given at the therapeutic dose of 12 mg/kg and RIF at 10 mg/kg reduced colony forming unit (CFU) to 4.5 and 4.3 log units in lungs, while the same doses of INH and RIF liposomes (Stealth®) reduced colony forming unit to 3.9 and 3.8 log units, respectively [20]. Labana et al developed liposomes containing an active targeting ligand O-steroyl amylopectin for encapsulation of RIF and INH. The formulation also exhibited a sustained drug release for more than 120 h, compared to 10 h for the free drugs and reduced the daily administration to only once a week [21]. Liposomes as nanocarrier drug delivery systems have also shown significant development in vaccines design for the treatment and prevention of TB. DNA vaccine combination expressing MTB heat shock protein 65 (HSP 65), IL-12, Ag85B-ESAT-6/CAF01 are the well-known examples of a vaccine liposomal-based technology with promising results [22].
(ii) Nanoemulsions
Nanoemulsions are defined as transparent or translucent water-in-oil (w/o) or oil-in-water (o/w) droplets with 10-100 nm mean droplet diameter [23]. Thermodynamically stable nanoemulsion of ramipril with mean particle size of 80.9 nm and polydispersity index of 0.271 was developed for oral administration. The relative bioavailability of ramipril nanoemulsion to that of conventional capsule and drug suspension were 229.62 and 539.49 %, respectively [24]. Ahmed et al developed various parenteral o/w nanoemulsions of RIF with excellent stability over 19 months [25].
(iii) Solid lipid nanoparticles
Back then in the middle 1990’s, Solid lipid nanoparticles (SLNs), the sub-micron colloidal carrier, were formally introduced as a novel drug-carrier system for oral deliver [26]. SLNs have captured enormous attention by various researchers and companies owing to the controlled drug delivery, enhancement of bioavailability of entrapped drugs and/or improvement of tissue distribution and targeting of drugs. There is a very less concern about their safety and biocompatibility as they are generally made from physiological lipids and surfactants [27]. Durgaramani et al designed RIF loaded SLNs with highest encapsulation efficiency of 78.79 % and in vitro release studies showed suitability of RIF-SLNs for the treatment of TB [28]. In 2013, Indu Pal Kaur incorporated RIF and INH into SLNs and studied the percent degradation of RIF in these combined SLNs (RIF-SLNs + INH-SLNs). The results showed increased bioavailability and prolong release of RIF by decreasing its degradation in presence of INH [29].
(iv) Polymeric nanoparticles
Most of the polymeric nanoparticles are bio-degradable and biocompatible and are preferred for the delivery of nano materials. Polymeric nanoparticles have been scrutinized to deliver a variety of antimicrobial agents to medicate various infectious diseases and have shown great therapeutic efficacy [30]. RIF, INH and STR loaded polymeric nanoparticles with elevated antimicrobial activity were prepared by Anisimova et al where encapsulated INH showed increased intracellular concentration of 4-8 folds, STR 7 folds and RIF 22-25 with respect to the extracellular concentration [31]. Correspondingly moxifloxacin loaded poly (n-butyl cyanoacrylate) nanoparticles delayed intracellular MTB growth at 0.1 µg/mL, whereas free moxifloxacin has same effect at 1 µg/mL [32]. Clemens et al employed meso-porous silica nanoparticle drug delivery systems either coated with a polyethyleneimine to release RIF or equipped with cyclodextrin based pH-operated nanovalves that open only at acidic pH to release INH into MTB-infected macrophages. Polyethyleneimine coated meso-porous silica nanoparticle demonstrated much greater loading and potency of RIF against MTB infected macrophages than uncoated. INH delivered by meso-porous silica nanoparticle killed MTB within macrophages more adequately than an equivalent amount of free drug [33]. To enhance the intracellular bioavailability of INH a highly hydrophobic citral-derived INH analogue named JVA was encapsulated in PLGA nanoparticles. Results suggested that JVA-NPs diminish pathogen proliferation and also increased MTB killing inside macrophages due to increase bioavailability of INH [34].
(v) Niosomes
Described as non-ionic surfactant vesicles having a bi-layer structure formed by self-assembly of hydrated surfactant monomers. Niosomes are delivering drugs directly to the body part where the therapeutic effect is required. This reduces the dose frequency to achieve the desired effects which subsequently decrease the side effects [35]. INH loaded niosomes were prepared by Roopa Karki. In vivo drug disposition study was evaluated in normal healthy albino rats. Niosomal drug delivery exhibited lower toxicity and less accumulation of drug than the free drug. The in vitro release pattern indicating sustained release for 48 h [36]. In 2011, Shubhini prepared INH niosomes which remained in the targeted site for longer time and also maintained INH concentration up to 30 h. The INH niosomes developed were capable of reducing drug dose and toxicity as well as dosing frequency which improved patient compliance [37]. In another study, Jain and Vyas developed micro-sized (8-15 μm) RIF loaded niosomes. It was revealed from in vivo studies that, depending upon the size of niosomes, up to 65 % of the drug loaded niosomes found in the lungs. The RIF niosomes had lower toxicity and were efficiently up taken into the lungs [38].
Furthermore, in 2010, Pavalarani studied niosomes of RIF and gatifloxacin. The bactericidal activities of the niosomal formulation were particularly examined using the resistant strains (RF 8554) and sensitive strains (H37Rv) of MTB. The results showed that these niosomes had greater inhibition and reduced growth index [39]. El-Ridy et al studied PYZ niosomes with maximum concentration in lungs, less side effects and decreased toxicity [40].
NEW ANTI-TUBERCULOSIS DRUG CANDIDATES IN CLINICAL TRIALS
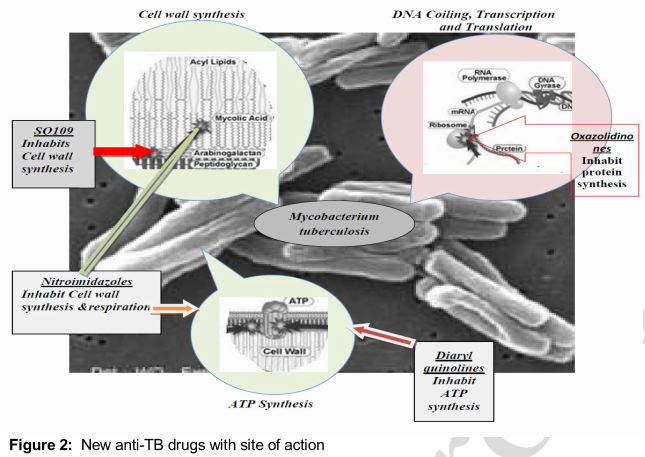
For the definite abolishment of TB; outdated drugs and regimens would offer no help. Instead there is a pressing need to make progress or development for new drugs but there are also some definite and comprehensible criteria for developing new TB drug candidates [41]. In addition to a fully confirmed safety profile, numerous other necessary factors should be fulfilled by a new anti-TB drug, that are: it should be more potent than existing drugs in order to reduce the duration of therapy; should inhibit new targets so that MDR-TB and XDR TB can be treated; be compatible with antiretroviral drugs; and show no antagonism to other TB drugs. Combining these new drugs with existing TB drugs revive hope for regimens that are better tolerated, shorter treatment duration and with less drug-drug interactions when compared with existing regimens For this purpose, various anti-TB drugs have been synthesized and tested in vitro [42] showed novel mechanism of action ().
These agents are expected to improve the treatment of drug-resistant, and possibly drug-susceptible TB used either separately or in combinations with standard therapy.
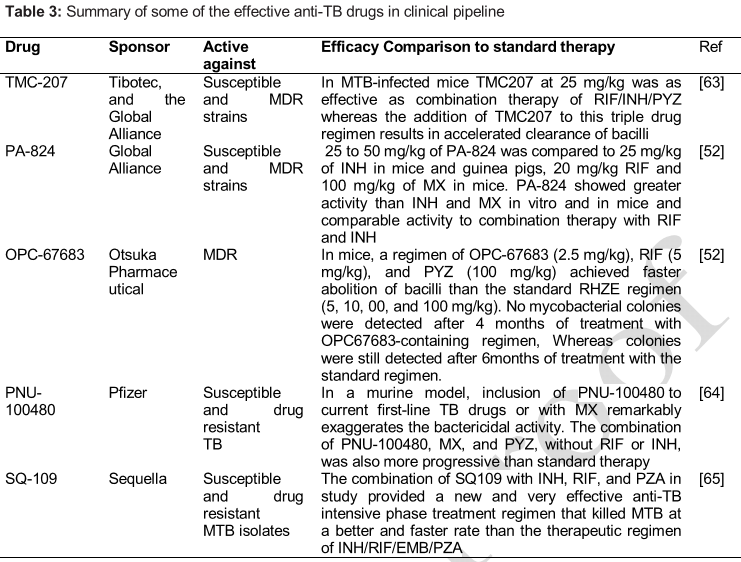
(i) TMC207
TMC207 formerly known as R207910 is the first anti-tubercular drug in the diarylquinoline class, with the MIC ranging from 0.002 to 0.06 μg/mL. In Phase II trials for the treatment of smear-positive pulmonary MDR-TB, TMC-207 was examined at 400 mg/day for 2 weeks, followed by 200 mg thrice weekly. It was found effective and safe [43]. In guinea pigs, TMC-207 was given for 6 weeks resulted in nearly complete elimination of MTB from body [44]. In 2008, Anil Koul has demonstrated an increased susceptibility of dormant mycobacterium toward TMC-207 as compared with actively growing bacteria. TMC-207 at 10 µg/mL was highly potent and killed dormant bacilli, as no bacteria could be detected by 14th day [45]. The remarkable activity of the combination of TMC-207 with PYZ in reducing the bacillary count by 5.6 log10 CFU after 1 month of treatment that is higher by more than 2 log10 CFU which obtained with the most effective drug combination without TMC-207, i.e., RIF-INH-PYZ [46].
(ii) Nitroimidazoles
Two new nitroimidazoles including PA-824 the lead compound from a series of nitroimidazoxazine derivatives and OPC-67683 (delamanid) the lead compound from a series of nitroimidazoxazole derivatives, are favourable drugs for TB. An early bactericidal activity study was performed to evaluate PA-824 orally at 200, 600 and 1000 or 1200 mg/day for 14 days. All doses were well tolerated, but unpredictably, showed comparable activity [47]. PA-824 exhibited significant anti-TB activity, with a MIC90 of 0.015-0.25 μg/mL against both drug-susceptible and resistant strains of MTB [48].
TB Alliance completed the clinical trial NC001, to evaluate combination of three-drug regimen PA-824, moxifloxacin and PYZ. The PYZ regimen presented substantially better effects than the standard treatment (HRZE) [49]. It is also markedly reassuring for MDR-TB patients who are susceptible to the drugs in the regimen, as it reduces the treatment from 2 years to 4 months together with being an efficiently economical and reasonable package costing just a fraction of the current MDR-TB treatment. It can be co-administered with common antiretroviral drugs, thereby improving treatment opportunity for patients co-infected with TB and HIV. PA-824 Studies in healthy volunteers showed a t1/2 of about 18 h and a time to reach Cmax of 4 to 5 h. About 65 % of drug is excreted in urine and 26 % in feces.
OPC-67683 is a nitro-dihydro-imidazooxazole and is closely related to PA-824. It inhibits the synthesis of methoxy and keto-mycolic acid, with MIC of 0.006 - 0.024 μg/mL and plasma half-life of 7.6 h. OPC-67683 shows potent anti-TB activity against both replicating and non-replicating bacteria and also against drug-resistant MTB. Therapeutic efficacy of OPC-67683 is evaluated in vivo in an experimental chronic TB mouse model, where OPC-67683 exhibited the most potent anti-TB activity in comparison with the reference compounds. A new regimen containing OPC-67683 could incomparably curtail the treatment extent by at least 2 months [50]. Killing activity of OPC-67683 was superior to INH and equal to RIF in an in vitro model of drug-tolerant MTB [51]. OPC-67683 was tolerated well by healthy volunteers at multiple doses from 5 up to 400 mg and no serious adverse effects were reported [52].
(iii) Oxazolidinones
(Linezolid, AZD5847 and PNU-100480) In addition to mycobacteria, Oxazolidinones possess a broad spectrum of antibiotic activity, against Gram positive aerobic and anaerobic bacteria [53]. Linezolid has demonstrated high in vitro antibacterial activity against MTB as well as MDR and XDR strains, with a minimum inhibitory concentration of less than 1 μg/mL [54]. Linezolid has been endorsed to be used at doses of 800 - 1200 mg/day in individual doses for the short-term treatment of bacterial infections [55].
Identical counterpart of linezolid, PNU-100480 is demonstrated slightly better in vitro activity. PNU-100480 proved to be well tolerated when given at a dose of 1,000 mg/day in healthy volunteers [56].
AZD5847 is another oxazolidinone to counterbalance the terrible cycle of TB, it is bactericidal and acts like linezolid. AZD5847 has similar MIC to linezolid and PNU-100480. It is well tolerated at daily oral doses of 800, 1600 and 2400 mg for 14 days in healthy volunteers with an increased Cmax of 10 µg/mL [57]. In another study, AZD5847 exhibited an MIC90 of 1 μg/mL and bactericidal activity of 2 μg/mL against both rapid-and sluggishly growing organisms when tested on MTB against laboratory strains and clinical isolates that are resistant to standard regimens [58].
(iv) Ethylenediamines (SQ109)
SQ109 is a 1,2-ethylenediamine ethambutol analogue [59] . In the mouse model, after an oral dose of 25 mg/kg, Cmax of SQ109 was approximately 0.14 μg/mL and the t1/2 of 5.2 h. After 28 days of treatment with 25 mg/kg of SQ109 or 100 mg/kg of EMB in MTB-infected mice, the lung CFU counts reduced by 2-log10, as compared to 3-log10 in control mice treated with 25 mg/kg of INH [60]. In 2012, Venkata studied bactericidal activity of PNU and SQ109 against MTB in vitro and in macrophages. Both compounds have an exemplary activity alone and in combination with other anti-TB drugs in chronic TB mouse models [61]. SQ109 has synergistic effect with INH, and RIF and it has also activity against EMB resistant strains in vitro [62]. In 2005, Protopopova unveiled the activity of SQ109 against drug-resistant strains of MTB. SQ109 was able to lower the intracellular MTB count by 99 % at its MIC of 1.56 mM. SQ109 demonstrated highest activity in vivo, mainly in lungs, and effective in curing TB infection in mice at 1 mg/kg while ethambutol at 100 mg/kg [59]. The list of TMC207, PA-824, OPC-67683, PNU-100480 and SQ109 drugs used as potent drugs to shorten the treatment of MTB is shown in .
Conclusion
Regardless of all the laborious measures and overtures taken for making the treatment a conducive procedure, TB never ceases to be one of the phenomenal challenging threats encountered at global level. The management of tuberculosis with anti-TB drugs chemotherapy dwells to be a difficult task. The cardinal reasoning for this is the development of resistance by microbes and severe uncertain blocks of conventional chemotherapy. Current therapeutic agents are life-saving for many patients, but fail to defeat MDR-TB/XDR-TB. The new anti-TB drugs are unquestionable needed to reduce the course of treatment, to compare against MDR- and XDR-TB and also to be easily administered in combination with antiretroviral drugs. Though identifying novel anti-TB agents remain a priority, the development of new formulations such as nano carrier systems to deliver existing anti-TB agents to the affected site is one of the alternatives to improve TB chemotherapy. Nano technology has a significant potential within the realm of possibility for treatment of TB, as it can improve drug bioavailability and reduce dosing frequency that may create a sound basis for better management of the disease. To top it all auxiliary anti-TB drugs offer the promise of shortened treatment regimens for drug-sensitive disease and more effective treatment for drug-resistant disease and latent infection, and also offer hope for future tuberculosis control.
Declarations
Acknowledgement
References
Archives


News Updates